Medicare Part D is Changing—Veradigm’s Response for Health Plans

Written by: Katie Wilson, Veradigm
Why Part D Matters to Health Plans
Medicare Part D is the prescription drug benefit for people with Medicare—and the administration of that benefit is changing.
Beneficiaries can enroll in a standalone prescription drug plan (PDP) or a Medicare Advantage plan that offers Part D coverage (MA-PD). Health plans whose members choose MA-PD become responsible for managing the CMS funding they receive for the population served. Changes in how Part D is funded can have a big impact on the bottom line of a health plan. In this article, we explore:
- The changes in Medicare Part D
- How Veradigm is responding to those changes with more resources
- The benefits of ongoing risk-adjusted analytics
What has Changed In Part D?
A donut hole has gone missing
The Centers for Medicare & Medicaid Services (CMS) recently announced changes to the Part D program for Calendar Year 2025. One notable change in this announcement is that the previous coverage gap—the “donut hole” where members became responsible for a larger portion of their prescription expenses—will no longer apply. Starting in 2025, each member’s out-of-pocket expense for Part D drugs will be capped at $2,000 annually. That means health plans will be liable for a greater portion of the claims expense than they had been previously.
A matter of increased liability
The Part D risk adjustment model has been updated to reflect the increase in liability that health plans will experience due to the benefit design changes. One modification to the Part D risk adjustment model is decreased coefficients for demographic components. This change provides the opportunity for health plans to emphasize confirming and validating the Part D condition risk scores to ensure those risk scores and their reimbursements are at appropriate levels.
How Veradigm Can Help Health Plans Adjust to Part D Changes
The change in the administration of Part D represents an industry shift. This will result in reduced cost burden for beneficiaries. That cost will instead be assumed by the health plan and, potential cost-sharing with the pharmaceutical supply chain. This may also increase access to medications that were previously out of beneficiary reach due to cost. These changes could potentially lead to adjusted pricing strategies, formularies, and cost-sharing.
Considering this shift, we have expanded our Risk Adjustment Analytics suite to help health plans identify opportunities to close revenue gaps in the risk-adjusted part of the revised Part D model.
Where Do Parts C and D Overlap?
Veradigm has extensive information for Part C members, which includes condition-level output files, intervention-targeting lists, efficacy of interventions, financial reporting, and dashboards. Because of the changes in prescription drug pricing, we will now supply this information for Part D members. We are focused not only on the Part D conditions that overlap with Part C conditions but, more importantly, the Part D conditions that do not overlap with Part C conditions.
Many Medicare Advantage-Prescription Drug (MA-PD) plans have historically placed a minimal emphasis on Part D in their risk adjustment programs as the majority of conditions in the Part D models are also found in the Part C models. That means plans that focus on Part C can still get the majority of what they need for Part D.
Health plans had believed that chasing the remaining Part D open gaps (conditions not yet coded) was not cost-effective relative to their return on investment. This approach had been sufficient in the past—prior to the current changes. But now, with increased dollars available for Part D, along with recent adjustments to the Part C models, Veradigm is responding to the changing dynamics in the Medicare Advantage risk adjustment landscape.
As Part C models shift from Version 24 (2020 CMS-HCC) to Version 28 (2024 CMS-HCC), the number of risk-adjustable diagnosis codes in Part C is reduced and will be fully effective in Payment Year 2026 (based on data collected from 2025 services rendered).1 Nearly 500 of the diagnosis codes being eliminated from risk adjustment consideration in the transition to Part C’s V28 model will remain in the Part D V08 model. Some conditions will have higher coefficient values in the new V08 model relative to the past.
With the increase in liability for Part D expenses, health plans must monitor Part D closely from both a revenue and an expense perspective to ensure that they can support their members in receiving the care and prescriptions they need.
Maintain Attention to Part D
Figure 1 shows that while there is significant overlap between the Part D model (V08) and the Part C models (V24 and V28), there are over 1,200 diagnosis codes that are either:
- Only Part D
- Currently, part of the V24 model will not be risk adjustable in the V28 model.
Although over 2,200 diagnosis codes from V24 will not be risk adjustable in V28, nearly 500 remain risk adjustable in Part D. Included in this list of risk-adjustable codes are endocrine/metabolic disorders, Diabetes with complications, coronary artery disease, and musculoskeletal disease. As Part D becomes more important to manage from a cost perspective, it will have less overlap with Part C than ever before.
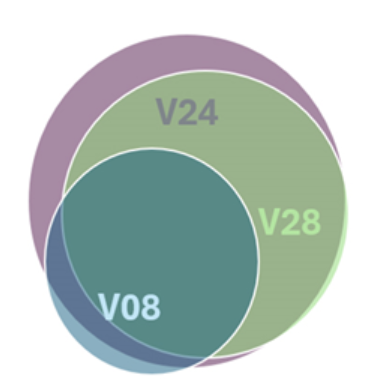
Figure 1. Diagnosis overlap between Part D and Part C version models.
Committed to Precise Risk Adjustment Analytics
Our preliminary results show that risk scores in the V08 RxHCC model for PY2025 are likely to increase for members who qualify as low-income due to the changes in the coefficients. Members who do not qualify as low-income will have lower risk scores than in the past.
Veradigm’s ongoing commitment is to precisely apply risk adjustment analytics to these CMS changes and other evolving markets. This commitment provides four key benefits2 :
- Periodically confirming the presence of chronic illnesses and preexisting health conditions in members, thereby ensuring that plans are adequately funded to care for their members
- Collating evidence, where it exists, to aid in the detection of unconfirmed, unsubmitted patient diagnoses—thereby ensuring that plans receive appropriate compensation
- Leading to earlier, more appropriate treatment of affected members by earlier detection of their health conditions
- Allowing precise, efficient targeting of risk adjustment interventions, thereby bringing health plans’ and healthcare providers’ attention to the right patients at the right time for the right reasons while simultaneously minimizing attempts at interventions that have a low chance of success
While we anticipate lower risk scores in Part D overall, we expect plans to increase Part D base rates to ensure they receive more funding to support their members and the prescriptions they need.
Veradigm Can Help Retain Revenue
The CMS move away from the “Donut hole” to capped out-of-pocket expenses from Part D Members represents the beginning of a shift toward health plans needing to absorb more costs. For that reason, it makes sense to pay careful attention to Part D revenue and expenses to ensure any revenue leaks are immediately found and stopped. Veradigm has a track record of successfully monitoring payment changes and can help you locate payment gaps you’ve been missing.
References:
- Shapiro JR. Department of Health & Human Services, Centers for Medicare & Medicaid Services. 2024 CMS-HCC Risk Adjustment Model Implementation and Update to Model Output Reports (MORs). Sept 1, 2023.
- Wrathall J, Belnap T. Reducing Health Care Costs Through Patient Targeting: Risk Adjustment Modeling to Predict Patients Remaining High Cost. EGEMS (Wash DC). April 20, 2017;5(2):4. doi:10.13063/2327-9214.1279.